

Insertion of a penile prosthesis is typically reserved as the last line of treatment for drug-refractory erectile dysfunction (ED). Loss of penile length as a result of penile prosthesis placement is the most common postoperative patient complaint shown to reduce overall satisfaction with the procedure.
The pathology behind the severe ED such as Peyronie’s disease, neglected ischemic priapism, loss of cavernosal smooth muscle and previous radical prostatectomy may have resulted in tunica scarring or fibrosis that severely limits the elasticity of the tunica albuginea. While not apparent in a flaccid penis, it becomes obvious after a penile prosthesis implant has been inserted and inflated.
Many patients who undergo insertion of a penile prosthesis may have a history of ED lasting many months or years. This could affect the accuracy of their recollection of what their penile sizes were prior to the onset of their condition.
An inflated penile prosthesis fills up only the corporal bodies of the penis and has no impact on glanular (tip of the penis) engorgement, which is a physiological phenomenon in normal erections. This lack of glanular swelling may contribute to the perception of decreased penile size.
Men who require penile prosthesis insertion are usually in the older age group. As a man ages or puts on weight, the fat in the prepubic region has a tendency to increase and engulf the penile shaft. This phenomenon of a partially “buried penis” may affect the patient’s perception of penile length after penile prosthesis implant.
As with other sexual dysfunction therapies, the outcome of penile prosthesis surgery is largely dependent on patient and partner satisfaction. Most frequent implanters will realize that perceived inadequacy of penile size, be it penile girth or penile length, are practical issues that need to be addressed in clinical practice, and may be best suited for a full discussion pre-operatively, to set realistic expectations.
Over the past two decades various techniques have been described in literature to address patient concerns. Some of these techniques can produce a measurable change in penile size, while others may merely work by producing a subjective perception of change, which nonetheless, is often sufficient to address patient concerns.
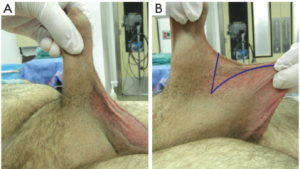
Ventral phalloplasty
In pediatrics, scrotoplasty has been used to improve the projection of an inconspicuous penis. Using the same principle, ventral phalloplasty, which involved the “check mark” excision of penoscrotal web (Figure 1) followed by reapproximation of the dartos along the axis of the penile shaft, has been performed at the time of penile prosthesis PPI to enhance the perception of greater penile length. In a study by Miranda-insertion. Patients who had ventral phalloplasty during PPI reported an increase in their perception of penile length 36/43 or 83% while only 2/43 (4.6%) patients reporting a decrease. This was compared to the response from 37 patients who did not have ventral phalloplasty during PPI, where 31/37 (83.8%) patients complained of penile shortening and only 1 (2.7%) reporting an increase in penile length.
The difference in patients reporting an increase in length compared to decreased length in both groups was statistically significant
Suspensory ligament release
Incision of the penile suspensory ligament allows the penis to drop into a more dependent position, giving a perceived increase in penile length. This procedure is commonly used in combination with inverted V-Y skin plasty.
Borges et al. released the penile suspensory ligaments of 303 patients who underwent implantation of IPPs via the infrapubic approach. There was no complaint of penile shortening in all the patients. Penile lengths of 18 patients were measured in a substudy before and after PPI. A mean increase of 2.4 cm flaccid penile length and 1.7 cm erect penile length was observed.
Upon implantation, the device was inflated and the penis pressed downwards. This allowed the fundiform ligament to be incised, so that the suspensory ligament can be exposed and detached from the pubis
To prevent reattachment of the suspensory ligament to the pubic bone, the implant was left partially inflated so that patient could apply downward pressure after surgery to maintain the distance between the pubis and the base of the penis. The use of a silicon spacer to prevent reattachment has also been described
Data on the therapeutic benefits of penile suspensory ligament release is currently inconclusive. Implanters performing this procedure as part of PPI surgery have to take into consideration the extended operative time, the risks of penile shortening from ligament reattachment contractures, the risk of wound infection and the potential complications associated with the use of a foreign body such as a silicon spacer.
Suprapubic lipectomy
In older men, weight gain together with changes in body fat deposition may cause the penis to be buried under excess skin of the panniculus, thus causing an apparent loss in penile length. Excision of the suprapubic fat pad with release of penile suspensory ligaments can create the perception of greater penile length.. In a team setting, where the plastic surgeon works alongside the urologist, suction lipectomy of the abdomen and pubic area combined with penile suspensory ligament release and abdominoplasty can yield satisfactory results .
Augmentation corporoplasty
Patch grafting is an established method to correct penile curvature in Peyronie’s surgery. In augmentation corporoplasty, tissue grafts are used to elongate the penis during PPI insertion. The use of synthetic materials, and treated biological materials have been described. Synthetic materials are less preferred because of the intense fibrosis associated with their use. Human autologous grafts are good options if longer operative time and donor site complications are not of major concerns. Treated biological materials do not require harvesting and are less likely to incite fibrosis, but they are generally more costly. Augmentation corporoplasty is not commonly done
Post-insertion strategies Other Section
The mechanical erections brought on by PPI are sometimes perceived as inadequate because of absent glans tumescence. This has a negative impact on patient satisfaction after PPI. To overcome this concern, intraurethral alprostadil, in the form of MUSE (medicated urethral system for erection) can be used with a functioning prosthesis to improve glans penis temperature, sensation and engorgement
Besides alprostadil, PDE5 inhibitors such as sildenafil have also been used to achieve this goal. In a study by Mulhall et al. 32 post-PPI patients reported a statistically significant improvement in satisfaction score when PPI is used in conjunction with sildenafil. The benefit arose mainly from better glans engorgement.
The use of intracavernosal injections and vacuum erection devices are generally not used after PPI surgery as there is an inherent risk of prosthetic cylinder damage. In some centers, subcutaneous injection of polyacrelamide gel into the glans are offered as a relief measure. Through one needle point, polyacrelamide gel is injected using a fanning technique and the injection site is sealed with 5/0 vicryl to prevent seeping of the gel and bleeding. The usefulness of glans injection is limited by its short-lived results (average 5 months).
If not yet done at the time of PPI insertion, ventral phalloplasty, suprapubic lipectomy and penile suspensory ligament release procedures can be contemplated as part of an overall post-insertion strategy to recover perceptual penile length.
Lee KCJ, Brock GB. Strategies for maintaining penile size following penile implant. Transl Androl Urol 2013;2(1):67-73. doi: 10.3978/j.issn.2223-4683.2013.01.05